by Anjali Joseph
I started my work in healthcare design research more than 16 years ago as a doctoral student at Georgia Tech working with Dr. Craig Zimring on synthesizing the literature on evidence-based healthcare design. This literature review and its follow up study published in 2008 clearly showed that the built environment of healthcare settings mattered in terms of improving patient safety, healthcare quality and patient experience. However, it also highlighted the complexity involved in studying healthcare environments and the difficulty in isolating the impacts of single built environment features from other factors such as patient characteristics, staffing and organizational factors. Over the years, I have come to realize that while it is important to conduct research focused around single built environment variables (e.g. light levels, door width) and healthcare outcomes (e.g. patient falls), it is perhaps even more critical to study and design healthcare physical environments as part of a larger work system. This is particularly true in high-risk patient care environments such as patient rooms, operating rooms and exam rooms that involve complex interactions between individuals, teams, tools and technology and the space where care is provided.
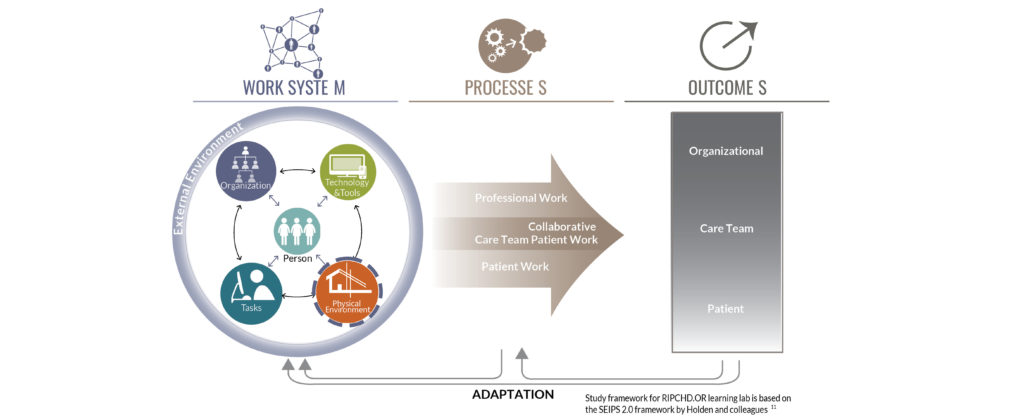
Existing frameworks in the health systems and human factors world recognize the physical environment as one of the components of the healthcare work system that impact healthcare processes and outcomes. These models such as the Swiss Cheese Model and the Systems Engineering Initiative for Patient Safety (SEIPS) framework suggest that the onus for providing safe patient care does not solely rest with the clinicians that interact with the patient. Rather, well-designed work systems are critical for achieving safe patient care. The work system as described by the SEIPS framework and others includes the physical environment, the people (patient, staff, families), the tasks performed, the tools and technology used as well as the organizational policies, that dynamically interact with each other over time to shape care delivery and healthcare outcomes.
While these models recognize the built environment as a system component, the physical environment is usually considered a given, hard to change, even while recognized as a significant barrier to care. Human factors researchers often focus on studying individual and team level interventions such as tools to support communication, or device and interface design to support physical and cognitive ergonomics, improve usability and reduce error. This body of research and practice recognizes the role of the physical environment in supporting healthcare work, but the interactions between the physical environment and other elements such as technology are understudied. For example, for one of our projects at the Center for Health Facilities Design and Testing focusing on integrating computer workstations in preoperative exam rooms, we found that while there were studies and tools around the physical ergonomics of the workstation itself and computer interface design, there was a lack of information about how these workstations should be integrated into the physical space of the exam room to support workflows and communication between clinicians, patients and families. This led us to develop an ergonomic assessment tool that focused on the integration of the workstation within the physical space. Similarly, several studies have identified clutter, crowding and noise as significant environmental challenges in operating rooms. However, we found that information on how the operating room physical environment layout and design supported the work of nurses, surgeons and anesthesia teams in ORs was lacking. This led to a multi-year collaboration as part of an Agency for Healthcare Research and Quality (AHRQ) funded patient safety learning lab on safe OR design resulting in a deep understanding of the OR work system, design of a new OR prototype and Safe OR design tool and implementation of our work in two ambulatory surgery centers.

It is challenging for healthcare architects and researchers to study complex healthcare work systems – they are difficult to access and observe, with a steep learning curve involved in understanding and interpreting what is observed. In this context, simulation-based evaluation of physical mock-ups are extremely helpful in obtaining input on work system performance. These evaluations engage frontline clinicians by asking them to simulate clinical tasks in typical and high-risk patient care scenarios using different equipment and technology. This allows staff to experience proposed designs within the context of their everyday work and identify physical environment features that pose challenges. For example, as part of the design process for a new 400-bed children’s hospital, the team at Children’s Healthcare of Atlanta built out a large warehouse with physical mock-ups for 11 clinical areas and conducted three rounds of simulation-based evaluations with more than 154 clinical staff. These evaluations focused on understanding the performance of the work system, resulted in significant design changes to address the 190 workflow and patient safety challenges identified. This project also highlights the importance of collaborating with clinicians, human factors and simulation experts in healthcare facilities to study and design these complex work systems.
A poorly designed healthcare work environment will create barriers to safe care every single day, while a well-designed and flexible physical environment can support the inherent variability of healthcare work. The healthcare facility design process for new buildings or renovations can be viewed as the design of multiple interconnected work systems at different spatial scales. These work systems will shape healthcare work and patient safety for years to come. It is important that healthcare design teams approach facility design projects from a health systems perspective, actively incorporating feedback from front-line staff using approaches such as simulation-based evaluation of physical or virtual mock-ups that allow the interactions between physical space, people, tasks and technology to be understood. Similarly, it is critical that healthcare organizations commit to incorporating questions and approaches related to the physical environment into all of their patient safety initiatives. The physical environment is a critical tool in the quality improvement and patient safety toolbox that is yet to be utilized to its full potential.
