This fall, I had the opportunity to work at the Center for Health Facilities Design and Testing as their first undergraduate intern. I am currently a senior here at Clemson University majoring in Health Science with a minor in Architecture. I had always wanted to work in the healthcare industry, so when deciding on a major, I went with the obvious choice. I had yet to learn how architecture is just as big a part of healthcare as anything else.
I decided to add a minor in architecture to my studies when I discovered the program my sophomore year here at Clemson. My roommate at the time was an architecture major and the work that she was doing fascinated me. I have always been interested in design and how our spaces can influence our behavior and how we think. The minor in Architecture introduced me to my love for architecture and completely changed my plans for the future. In order to complete my bachelor’s in health science, we must finish an internship in the field, and I think I was the first to tell my advisor that I wanted my internship to be related to architecture. She did some research and was eventually able to connect me to the Center for Health Facilities Design and Testing (CHFDT), a perfect mix of my two interests. I reached out to Anjali, the Director of the Center, and expressed my interest in working with them and was thrilled to be selected as their first undergraduate intern.
The CHFDT has given me a unique perspective on what a future in healthcare can look like. When I first walked into the Center, I didn’t know what to expect. As the Center’s first undergraduate intern, I was excited to see what I was going to work on and how health and architecture interact. During my internship, I have had the opportunity to assist the team with the EDen room project, which is focused on designing a flexible emergency department room for mental and behavioral health patients, as well as medical patients. My roles have included sitting in on team meetings, collecting data from mental health professionals during simulation-based evaluation of physical mock-ups, and analyzing that data to develop recommendations for design refinement. I have learned about the importance of minimizing ligature risks for mental and behavioral health patients and how lighting, color, and the overall design of the physical environment can improve comfort and support patient dignity.
One of the most rewarding parts of this experience has been being surrounded by such a talented team, including PhD students, researchers, and architecture students. They’ve introduced me to research methods that have deepened my understanding of how healthcare spaces affect patients and staff. I’ve learned how to formulate research questions, analyze data from behavioral observations, and gather feedback through interviews and mock-up simulations. It was interesting to see how insights from staff can affect design and how we can use that data to support patient and staff safety.
Some highlights of my time here at the Center include our pumpkin carving event for Halloween where we all got to showcase our design skills on pumpkin faces and acting the role of a patient being transported in a hospital as part of a training exercise for a research study on intrahospital transport. I was transported around in a wheelchair by PhD students playing the role of nurses with a trashcan as my oxygen unit, while other researchers tested out the tools they were going to use for the actual study at Children’s Healthcare of Atlanta. The team has truly welcomed me as one of their own and have taught me valuable skills that I will take with me wherever I go.
Overall, this internship has helped me discover a new perspective on health and design and how my interests can be combined. I love thinking about how spaces can impact behavior and how design can improve healthcare experiences. I am grateful to have had the opportunity to be the first undergraduate intern with the CHFDT and to have been able to figure out together with the team how undergraduate students can potentially assist in future research projects. As I move forward, I plan to pursue a Master of Architecture and continue to explore how design can support health and create environments where patients and caregivers can feel safe. This experience has helped me decide what I want my future to look like in the healthcare industry and I am excited to see what more I can learn with my time left at the Center.
The Architecture + Health program was fortunate
to have the opportunity to travel to New Orleans, LA to attend the 2023 HCD
conference. In addition to attending the HCD Conference, we were also able to
see the National Memorial for Peace and Justice in Montgomery, Alabama, meet
some wonderful alumni of the A+H program, and tour two inspiring hospitals as
well as the HKS Atlanta office.
Our first stop on Thursday was the Northeast
Georgia Medical Center, where we had the opportunity to tour the mechanical
spaces and learn about the mechanical systems that enable this hospital’s energy efficiency. In the evening, we were
joined by alumni Chenyue Yuan for a wonderful dinner.
We began our day on Friday with a wonderful
experience touring the HKS Atlanta office. The team was hospitable and the
office was beautiful, and it was a great experience to get an insight into such
a respected firm in healthcare architecture. We are so grateful to our A+H
alumni and the whole team for their hospitality, and for taking the time to
share some projects and experiences with us.
The National Memorial for Peace and Justice
aims to create a space to for people to gather and reflect on our nation’s history of racial inequality in a sober and
meaningful way. The memorial is constructed with over 800 steel monuments, each
representing a county in the United States where a lynching occurred, and the
names of victims are engraved on the columns. As we explored this deeply moving
space, we experienced the power of architecture to express grief and memory,
and to inspire change.
On Saturday, we had the opportunity to tour the
New Orleans Children’s
Hospital. This was a valuable and wonderful experience to expand our
understanding of pediatric hospital design. It was a great privilege to have
this tour of such a beautifully designed facility.
On Monday night we were joined by over 50 A+H
alumni and had a fantastic time meeting and reconnecting!
We had three wonderful days at HCD, attended
many extraordinary lectures and seminars, connected with many inspiring people,
and returned home looking forward to implementing some new ideas into our
projects. We were able to be present for presentations from Clemson Professors
David Allison, Anjali Joseph, Dina Battista, and Vincent Blouin. Several A+H
alums were recognized for exemplary contributions in healthcare architecture.
Congratulations to the following A+H alumni who received recognition at HCD 2023!
Presentations:
David Allison
Anjali Joseph
Dina Battisto
Vincent Blouin
Anthony Asher
Christian Bormann
Scott Meade
Kimberly Stanley
Deborah Wingler
Kirk Hamilton
Walter B. Jones
Frank Zilm
Asma Sanaee
Shan Jiang
MillerKnoll:
Madilyn Dubois
Cassidy Bland Roberts
Tuttle Fellowship:
Sara Kennedy
GMZ Fellowship:
Swati Goel
2023 Healthcare Design Awards:
Kenneth Webb (HKS)
Kimberly Bandy (ZGF)
David Allison
Anjali Joseph
HKS Atlanta
alums:
Thabang Nyondo
Les Saunders
Hannah Shultz
Ethan Hopkins
New Orleans Children’s
Hospital:
Sarah Wade Walter
What an incredible experience, and a truly
unique opportunity for us as students to attend a trip like this. We are
sincerely grateful.
The No Place to Play exhibition focuses on specific findings about gender taken from a large research study with the same name. The larger study was conducted by Dr. Lyndsey Deaton, a Professor of Architecture in the Architecture + Health program at Clemson University. The project links economic development policies to social inequality in gentrifying communities in South and East Asia by highlighting how spatial changes affect teenagers’ mobility and access to public space. The forthcoming book (2024) is written for concerned parents, policymakers, designers, and community advocates. In it, Dr. Deaton describes five years of living alongside seven dispossessed communities and builds a case for contextualized, community-driven design.
Dr. Lyndsey Deaton Opening the show
The exhibition was designed and constructed by a group of Clemson University students from a variety of majors including architecture, psychology, women’s leadership, and sociology led by Dr. Deaton. It is an artistic demonstration of the influence gender has on teenagers’ access to public space in post-displacement communities. The exhibition highlights 50 teens from seven communities in India and the Philippines. Walking through this exhibition, visitors will hear recorded conversations with teens and see maps and photographs they created to better understand how displacement affects teen socialization. Finally, join our team of Clemson students in considering the similarities between the teens’ experiences in this study and the urban public spaces around South Carolina.
Exhibition Window PlacementWhere the Third Place is
Maternal care was an early clinical interest for me and this interest inspired me to pursue nursing so many years ago. As a student in the certificate program in Leadership and Innovation in Health + Design at Clemson University, I am enjoying studying the connections between healthcare policy, nursing and the design of the built environment. Last semester, I had the opportunity to undertake research on an area of public health policy and explore its connection to the built environment. I chose to study maternal mortality and morbidity and its relationship to the design of the built environment. In conducting the research, I was saddened to see the trends in the U.S. and feel called to do what I can in my new career, blending my extensive experience in healthcare with planning, design and construction to make a difference through the built environment.
I learned that the maternal mortality rate in the U.S. has risen consistently since data collection began from 7.2 deaths per 100,000 in 1987 to 17.3 in 2017. The maternal death rate exceeds that of 40 other countries and the U.S. is one of only eight countries worldwide and the only developed nation where maternal mortality has actually increased over the past three decades. Additionally, for every maternal death there are estimated to be 70 cases of severe morbidity, and many more near misses that are not quantified. With up to 60% of maternal deaths being categorized as preventable, there has been heightened interest in the clinician, patient and institutional factors that contribute to poor maternal outcomes, and to identify potential areas for intervention.
While there is a large body of literature outside of obstetrics linking care environment with patient outcomes, there is limited research on the impact of the physical environment of obstetric care on maternal morbidity and mortality. What I did learn from the limited research found on birth environments, is that there are three important built environment themes which promote normal physiological birth processes, influence the need for medical interventions, and effect cesarean section rates. The three areas that architects, clinicians and healthcare administrators should consider for design and research in birth settings are the overall aesthetics of maternal care environments, the design of the birth room as well as unit layout and design. These influences, in turn, impact maternal mortality and morbidity, both directly and indirectly.
Aesthetics
The overall aesthetics of the birth experience are important in helping to avoid triggering a fear cascade in the laboring woman, which is known to affect the birth processes by disrupting the normal physiological hormonal response in labor. The aesthetics of the space are extremely important and include all the areas the woman will encounter throughout hospitalization, and should be designed to promote relaxation. Included are the use of warm colors, textured surfaces, a homelike look for furnishings and fabrics as well as the use of soft lighting, natural light, and views of nature. Artwork, posters or symbols using the female archetype, located in strategic places in birth rooms or the unit where the laboring woman might walk, have been shown to be calming and helping to decrease stress.
Birth Room
The birth room contributes to the normal physiological processes of labor. Labor progressing naturally on its own lessens the need for medical interventions. In addition to the birth room aesthetics, birth rooms must have the essential technical equipment such as fetal monitoring capabilities and neonatal care equipment immediately available. However, for some, its’ presence might trigger anxiety or fear, so housing it in concealed cabinetry unless needed is recommended. Similarly, access to emergency supplies in the room is essential to prevent delays in necessary care, but like other technical equipment, should be concealed whenever possible. Another aspect that can trigger the fear cascade is lack of privacy. The spatial filter, which is the interface between the public corridor and the room itself, is a design element to consider. Privacy curtains, half walls, or doors angled in a way that protects the inside of the room from view from the hallway can be utilized to enhance the sense of privacy.
Features of the birth room layout contribute to the normal physical mechanisms of labor. The room’s size, shape and layout configuration should allow for flexibility to change the room for the different phases of labor and to facilitate the woman utilizing the space in a way most comfortable for her. The laboring woman needs to be able to move around and assume varied positions, so having space for optimal equipment such as birthing stools, bean bags, gym mats, wall bars, along with accessible bathrooms with showers and birthing tub is necessary. The amount of time the woman spends lying in bed impacts the progression of labor (less being better), therefore, the ability to easily move the bed out of the way should be factored into the design. Because continuous labor support is linked to successful outcomes of labor, having sufficient space in the labor room for the supporter and their belongings should be prioritized. Lighting and temperature of the rooms should be capable of being controlled by the woman and or her supporter.
Unit Layout/Design
Beyond the spaces that the laboring woman encounters during the birth process, the overall unit layout has important implications for minimizing morbidity. Because obstetric hemorrhage is a leading cause of maternal death and morbidity, managing hemorrhage requires ready access to life-saving equipment, medications and blood products. In particular, birth units should regularly reassess current practices, logistics, and locations of blood products relative to where they might be needed. At “baseline” blood storage be in the same building as the labor unit, but a “better” practice would be storage on the same floor, and “best” practice would be storage of blood product right outside the cesarean section operating room.
Additional insight into the importance of unit layout emerged from the Ariadne Lab and Mass Design Group’s exploratory study linking facility design with cesarean section rates. High cesarean rates having been identified as a key factor in the increasing maternal morbidity and mortality rates. They concluded that more deliveries per labor room, fewer labor rooms per operating room, higher ratio of overflow beds to labor rooms, longer distances between spaces, proximity of on-call rooms, and lower percent of support areas designated as collaborative spaces, were all associated with higher cesarean delivery rates. Limited unit or facility capacity, high workload, and limited accountability for decision–making all contribute to the clinical decision to perform a cesarean section. Normal vaginal delivery is both space and clinical resource-intensive, whereas a cesarean delivery requires only a few hours of clinical attention. When under pressure to make more space for incoming patients, or in times of staffing shortages, a decision point of whether to continue to attempt vaginal delivery or expedite things by performing a cesarean birth is reached. Thus, design elements can play a significant role in that decision.
Conclusion
Despite the limited number of robust studies on the built environment for labor and delivery, the research that exists supports the essential role of the built environment in promoting physiologic labor processes and reducing maternal morbidity and mortality. These initial studies provide some direction for healthcare planners and designers. However, further research is much needed! Looking to the practices and processes from other countries who have succeeded in reducing the alarming mortality and morbidity rates should also be pursued.
The Environmental Design Research Association came into being in the 1960s, led by a group of forward-thinking activists and environmental design researchers who believed that architects and designers held a social responsibility to create environments that supported human behavior and intentions, well-being and performance for everyone. This highly multi-disciplinary and inclusive community includes psychologists, social science researchers, architects, landscape architects, interior designers, design researchers and students with a range of interests and focus areas. EDRA members represent many different countries and are leaders in the field of environment and behavior studies, evidence-based design, facility evaluation methods, sustainability, active living, participation, community planning, universal design, diversity in design, workplace design and informatics, design education, and digital technologies. Anyone interested in engaging in conversation around the design of the physical environment and its impacts on human behavior and performance has a home in the EDRA community.
I first attended EDRA in 2003 as a doctoral student at Georgia Tech. I vividly recall standing nervously in front of my poster during a session at EDRA. I remember the many friendly EDRA members who stopped by to provide words of encouragement and advice. At another EDRA conference, at the urging of my advisor Craig Zimring, I organized a workshop session on active living for environments for aging. With Craig’s support, I was able to recruit many leading EDRA researchers including Habib Chaudhury, Atiya Mahmood, Benyamin Schwarz and Gerald Weisman. As I found then and it continues to be the case, the EDRA community is generous in sharing their knowledge and willing to mentor and support young students and early career professionals. These interactions and countless others at EDRA helped me gain confidence as a speaker and researcher and helped me make connections that have served me well during my career.
EDRA creates so many opportunities for students and professionals to enrich their careers and expand their knowledge about environmental design, just like it did for me as a student. The values and philosophy of EDRA resonates with so much of what we do at the Clemson School of Architecture and the Center for Health Facilities Design and Testing. For all these reasons and many more, Clemson University and EDRA 53 co-chairs (Dina Battisto, B.D. Wortham- Galvin and I) are deeply honored and excited to be hosting the 53rd Environmental Design Research Association (EDRA) Annual Conference in 2022 in Greenville, SC!
The theme of the 2022 conference is Health in all Design: Promoting health, equity, sustainability and resilience through environmental design. As we emerge from a global pandemic, it has become imperative that environmental designers and researchers consider health – a state of complete physical, social and mental well-being over time – as a critical goal for all design projects. The pandemic has highlighted the importance of the built environment in promoting safe and healthy lifestyles by providing access to outdoors and green areas for physical activity, good air quality and building layouts that support hygienic practices indoors, and ergonomic design that promotes wellness in workplaces. The pandemic has also highlighted stark inequalities – black, indigenous and people of color (BIPOC) communities have been disproportionately impacted in terms of mortality, illness and unemployment. Providing access to safe and affordable housing, healthcare and health-promoting resources has never been more critical for these communities. Greenhouse gas emissions resulting from human activity including transportation, building construction and operation are contributing to climate change, and future designs should not only impact individual and community health but also help improve planetary health. Inclusive of sustainability and cities’ abilities to help sustain diverse environments, cultures, and economies locally and globally, resiliency which implies the ability of a community to anticipate and recover from challenges is needed now more than ever before. Through ‘Health in all Design’, EDRA 53 will bring together a multidisciplinary community of practitioners and researchers to engage in a conversation about the role of built environment in promoting health, equity, sustainability and resilience as we move beyond the pandemic.
Greenville is a prime example of our proposed theme: Health in all Design. Through an engaged public private partnership, the city of Greenville was revitalized to include a range of health-promoting community resources including walking and biking trails and parks such that it is listed among the 10 most livable cities in the US. Further, the city plans to implement smart city concepts in the near future to support health and well-being of its residents. Clemson University’s College of Architecture, Arts and Humanities (CAAH) and its allied programs that are encompassed by EDRA – landscape architecture, city planning, historic preservation, architecture and health, and resilient urban design – are deeply engaged in conversations locally and globally around health, equity, sustainability and resilience. The Interdisciplinary Ph.D. program in Planning, Design and the Built Environment (PDBE) in CAAH also includes a concentration in Built Environment and Health. The graduate program in Architecture + Health at Clemson focuses on studying how architectural environments impact health and how to create architectural settings that support the health and well-being of individuals and larger populations. The Master’s program in Resilient Urban Design (MRUD) prepares individuals to engage complex cultural, market, and government policy forces through sustainable and resilient urban form. Further, we integrate professional degree programs and research programs to foster lively discussions around blending design, theory and practice. The focus of these programs as well as the broader mission of the landscape architecture and architecture programs at Clemson align well with the goals of EDRA and the theme of this conference.
This proposed theme invites abstracts that focus on research, projects, methods, and designs that envision a safer and healthier post-pandemic world. Thus, the theme will manifest in various session tracks that might include:
Health, Equity, Resilience and Sustainability: How are we generating knowledge to address the great challenges of the time, like: public health issues, an increasingly digital society, climate change, social inequities, overpopulation, stewarding tangible and intangible heritage, an increase in both waste and pollution (soil, air, noise, water), natural resource depletion, access to affordable housing, access to food and water, loss of biodiversity, loss of cultural diversity, urban sprawl, etc.? How do we rely upon simultaneity and adjustability to manage these challenges both locally and globally?
Designing for Diverse Populations: How are we considering the needs of post-pandemic? What impacts did our buildings, communities and natural environments have on vulnerable populations including children, ethnic minorities, young adults, the elderly, people with mental disorders, people with physical disabilities during the pandemic? How will the lessons learned during the pandemic shape the design of future environments for diverse populations?
Designing for Health: How do design and planning professionals approach and define health and well-being as a core part of their practice? How does it affect their methods? What are the emerging design tools (data, simulation, virtual) and how are they being deployed in design projects?
Activism & Advocacy: What are the methods, conversations, and outcomes for those researching and designing under the auspices of design activism, action research, public service, and public education? We encourage not only success stories but also critical discussions of pitfalls and “failures” that serve as learning opportunities for this work.
Trans-disciplinary: How are professionals and academics crossing boundaries to address emerging issues of health, equity, sustainability and resilience in a post-pandemic world? What are the means for doing this? What critiques emerge when blurring and/or borrowing from multiple disciplines?
Pedagogies/Methods: What are the ways in which teaching promotes design and research excellence, innovation, and/or activism? What methodologies are being embraced by environmental design faculty in order to innovate and stimulate their research? How are emerging design tools (data, simulation, virtual, etc.) being used in the classroom and/or in research?
Join us June 1-4, 2022 to discover more about ‘Health in all Design’ and what we can learn from experts in environmental design. EDRA holds a special place in my heart and I am very excited to bring EDRA to Greenville and Clemson. To get involved with EDRA events, explore publications, and expand networking opportunities click here.
Approximately 187,000 students enroll in a Ph.D. program each year in the United States. My journey is specific to Clemson University’s Planning Design and Built Environment cohort of 2023, with a concentration in Architecture + health during COVID-19 times. I would say that makes it quite unique.
I am an international student from India. I am trained as an architect. My research interest brought me to the United States in 2017 to get a master’s degree in design and health from the University of Michigan. I started my Ph.D. program at Clemson in the fall of 2020 after working as an architect for two years (to ensure I was making the correct decision for my career). I am passionate about architecture and mental health and was looking to combine design and research. That is when I stumbled upon Clemson’s Architecture + Health program.
COVID-19 hit the United States hard a year ago in March of 2020 and slowly took away all sense of community and peer support. Initially, I thought it would allow me to focus better. Still, as time went by, physical distancing began to feel exhausting, and there was no one to share the good and the bad. I had moved to South Carolina from Indiana after quitting my job as an architect and leaving behind all my friends and support system. COVID-19 made it hard to establish new connections at the onset, a crucial ingredient of graduate school.
The first semester at Clemson University was a significant change and called for adjustment. I had moved multiple times before, but this time was different with no previous acquaintances. Besides, shifting my mindset from an Architectural Designer to a full-time researcher was exceptionally challenging. It required a complete rehauling of my approach towards work. While designing, architects constantly improvise a set of drawings or writing guidelines, which can be reused and do not need a systematic process. However, research is very organized and novel. The process is unique and requires constant reading and insight. The first two months went into decorating my new apartment, but once that was done, all I had left was my studies and an endless series of ZOOM calls. Three months into it, I realized there was a term for it- ZOOM fatigue! (Fauville et al., 2021)
All the classes were online, research assistantship work was online, and all my friends and family were online. I could not meet people and make many new friends in Clemson. A few months into the program, my advisor suggested that the research assistants work in the Ph.D. student offices while practicing social distancing. It was nice to leave my house and be around my research team once or twice a week. I was beginning to see the importance of peer support while pursuing a Ph.D. We could talk through ways of doing research activities and brainstorm ideas. It is tempting to stay home and sit in front of the computer and plan and read. However, once I started going to school, I realized the importance of in-person interaction, taking breaks, and investing in myself; instead of just being a Ph.D. student. In a study assessing the effects of the COVID-19 pandemic on college students’ mental health conducted at a large university in Texas, 86% (n=195) of the participants reported decreased social interactions due to physical distancing, while 89% reported difficulty in concentrating (Son et al., 2020).
I grew more and more grateful for the support system I found in the other Ph.D. students who I had the opportunity to meet and work with in person. Earlier I used to think that a Ph.D. is a feat to be accomplished alone, but it is the opposite. The more we alienate ourselves, the harder it gets. It needs to be shared and celebrated, at least the first two years! That’s how we grow as individuals and researchers. It gets better. In the Fall of 2020, the Center for Health and Facilities Design Testing (CHFDT) team organized multiple (physically distant) events such as pumpkin carving on Halloween and hikes in nature to enforce peer connection. Clemson University held socially distant football games at the memorial stadium with reduced seating. And finally, in my winter break, I celebrated Christmas with my fabulous new friends in Clemson and later saw my friends in Indiana. These activities reinforced the importance of combining work and play and the power of community and peer support.
I am in my second (spring) semester right now. The expectations are higher, but I feel more at home with myself. I have a nice routine. I am more organized. I am more in sync with my role as a researcher. I have a great support system within my research community and outside. I reach out to my friends and mentors whenever I need them. I am more productive and yet carve time to be myself.
All research papers end with a conclusion! A year later, and COVID-19 hasn’t left our lives; in fact, it has been a unique experience for everyone. Students and professionals are suffering due to more than usual hours spent at home. Clemson’s dining halls are open this spring, and I think the line between sweatpants and jeans is blurred. Screen time has increased, and exposure to sunlight and physical activities plummeted, leading to a rise in mental health issues. In the research at a Texas University, only 76% (105/136) of students utilized any coping mechanisms to handle the stress due to the outbreak (Son et al., 2020). Out of these 105 students, only 30% of students mentioned using physical exercise to manage stress. Another 21% used streaming and social media as a means of self-management. 44% of the students experienced some depressive thoughts due to loneliness and uncertainty. These outcomes worry me, and I wonder how an architect + researcher would respond to that? I do not have a perfect answer, but I am looking.
Personally, COVID-19 taught me to be grateful for my peers and colleagues. I am thankful for a supportive and encouraging team at the Center for Health and Facilities Design Testing. I am thankful to my advisor for thinking ahead of time and encouraging us to return to our offices while being safe. These experiences made me humble and appreciative of little things that I would not have if I were not forced to spend so much time alone. Maybe there is a lesson for all of us here!
Sources:
1. https://www.statista.com/statistics/185167/number-of-doctoral-degrees-by-gender-since-1950/
2. https://news.stanford.edu/2021/02/23/four-causes-zoom-fatigue-solutions/
3. https://cookchildrens.org/coronavirus/action/Pages/Safe-Reopening.aspx
4. Son, C., Hegde, S., Smith, A., Wang, X., & Sasangohar, F. (2020). Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. Journal of Medical Internet Research, 22(9). https://doi.org/10.2196/21279
5. Fauville, G., Luo, M., Muller Queiroz, A. C., Bailenson, J. N., & Hancock, J. (2021). Nonverbal Mechanisms Predict Zoom Fatigue and Explain Why Women Experience Higher Levels than Men (SSRN Scholarly Paper ID 3820035). Social Science Research Network. https://doi.org/10.2139/ssrn.3820035
I started my work in healthcare design research more than 16 years ago as a doctoral student at Georgia Tech working with Dr. Craig Zimring on synthesizing the literature on evidence-based healthcare design. This literature review and its follow up study published in 2008 clearly showed that the built environment of healthcare settings mattered in terms of improving patient safety, healthcare quality and patient experience. However, it also highlighted the complexity involved in studying healthcare environments and the difficulty in isolating the impacts of single built environment features from other factors such as patient characteristics, staffing and organizational factors. Over the years, I have come to realize that while it is important to conduct research focused around single built environment variables (e.g. light levels, door width) and healthcare outcomes (e.g. patient falls), it is perhaps even more critical to study and design healthcare physical environments as part of a larger work system. This is particularly true in high-risk patient care environments such as patient rooms, operating rooms and exam rooms that involve complex interactions between individuals, teams, tools and technology and the space where care is provided.
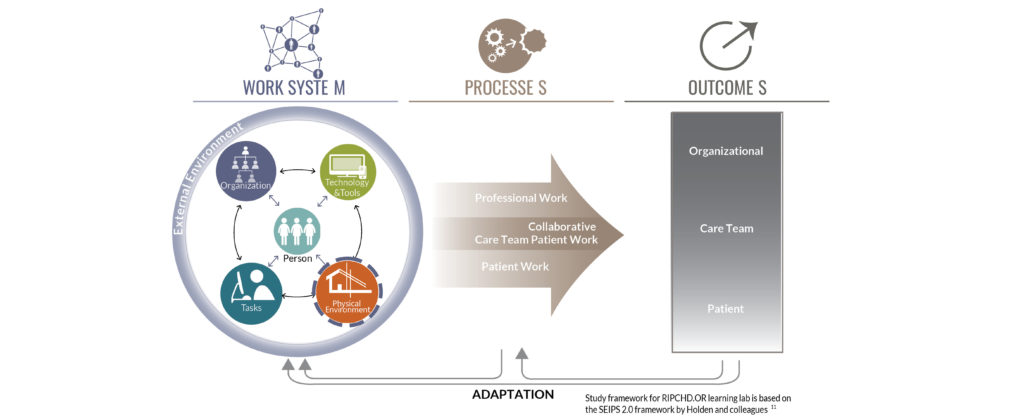
Existing frameworks in the health systems and human factors world recognize the physical environment as one of the components of the healthcare work system that impact healthcare processes and outcomes. These models such as the Swiss Cheese Model and the Systems Engineering Initiative for Patient Safety (SEIPS) framework suggest that the onus for providing safe patient care does not solely rest with the clinicians that interact with the patient. Rather, well-designed work systems are critical for achieving safe patient care. The work system as described by the SEIPS framework and others includes the physical environment, the people (patient, staff, families), the tasks performed, the tools and technology used as well as the organizational policies, that dynamically interact with each other over time to shape care delivery and healthcare outcomes.
While these models recognize the built environment as a system component, the physical environment is usually considered a given, hard to change, even while recognized as a significant barrier to care. Human factors researchers often focus on studying individual and team level interventions such as tools to support communication, or device and interface design to support physical and cognitive ergonomics, improve usability and reduce error. This body of research and practice recognizes the role of the physical environment in supporting healthcare work, but the interactions between the physical environment and other elements such as technology are understudied. For example, for one of our projects at the Center for Health Facilities Design and Testing focusing on integrating computer workstations in preoperative exam rooms, we found that while there were studies and tools around the physical ergonomics of the workstation itself and computer interface design, there was a lack of information about how these workstations should be integrated into the physical space of the exam room to support workflows and communication between clinicians, patients and families. This led us to develop an ergonomic assessment tool that focused on the integration of the workstation within the physical space. Similarly, several studies have identified clutter, crowding and noise as significant environmental challenges in operating rooms. However, we found that information on how the operating room physical environment layout and design supported the work of nurses, surgeons and anesthesia teams in ORs was lacking. This led to a multi-year collaboration as part of an Agency for Healthcare Research and Quality (AHRQ) funded patient safety learning lab on safe OR design resulting in a deep understanding of the OR work system, design of a new OR prototype and Safe OR design tool and implementation of our work in two ambulatory surgery centers.
Floor plans with cone of vision from care team member to care partner and patient in a preoperative workspace. Sourced from the Ergonomic Assessment Toolkit.
It is challenging for healthcare architects and researchers to study complex healthcare work systems – they are difficult to access and observe, with a steep learning curve involved in understanding and interpreting what is observed. In this context, simulation-based evaluation of physical mock-ups are extremely helpful in obtaining input on work system performance. These evaluations engage frontline clinicians by asking them to simulate clinical tasks in typical and high-risk patient care scenarios using different equipment and technology. This allows staff to experience proposed designs within the context of their everyday work and identify physical environment features that pose challenges. For example, as part of the design process for a new 400-bed children’s hospital, the team at Children’s Healthcare of Atlanta built out a large warehouse with physical mock-ups for 11 clinical areas and conducted three rounds of simulation-based evaluations with more than 154 clinical staff. These evaluations focused on understanding the performance of the work system, resulted in significant design changes to address the 190 workflow and patient safety challenges identified. This project also highlights the importance of collaborating with clinicians, human factors and simulation experts in healthcare facilities to study and design these complex work systems.
A poorly designed healthcare work environment will create barriers to safe care every single day, while a well-designed and flexible physical environment can support the inherent variability of healthcare work. The healthcare facility design process for new buildings or renovations can be viewed as the design of multiple interconnected work systems at different spatial scales. These work systems will shape healthcare work and patient safety for years to come. It is important that healthcare design teams approach facility design projects from a health systems perspective, actively incorporating feedback from front-line staff using approaches such as simulation-based evaluation of physical or virtual mock-ups that allow the interactions between physical space, people, tasks and technology to be understood. Similarly, it is critical that healthcare organizations commit to incorporating questions and approaches related to the physical environment into all of their patient safety initiatives. The physical environment is a critical tool in the quality improvement and patient safety toolbox that is yet to be utilized to its full potential.
What has it really been like in architectural practice, education, and research during the pandemic? The way we work changed overnight in 2020. In this article, we share insights from Architecture + Health students, researchers, practitioners, and colleagues.
Communication with Clients
Previously our workdays involved a variety of formal and informal interactions with our clients, in person as well as via phone, voice message, email, text, or video conference. In-person interaction and on-site visits have been replaced by digital communication. This has changed the nature of communication for everyone sensitive to the need to prevent zoom fatigue and engage clients meaningfully. However, in the absence of in-person interactions, there is still the need to build and maintain relationships. The challenge is to communicate effectively and succinctly while also providing value and building trust with the client. Deborah Wingler, PhD, Health and Research lead at HKS in Dallas, TX says “We need to be really thoughtful about what information we are giving and how we are giving it. Maybe before COVID we would just send a quick email or message. Now it might be better to engage with a personal call or video chat to try to maintain personal connections.” Deborah observed that busy health care clients today often appreciate the shorter and more efficient meetings that can be held virtually in less time than larger in-person sessions.
Communication in the Classroom
As a Gen-Xer who did hand-drafting in design studio for my Bachelor of Architecture degree, one of the biggest changes I noticed with the transition to digital tools in the early 2000’s was that students were less able to share their work and discuss ideas with others. Returning to school 25 years later, my first semester pre-pandemic was very different from the undergrad experience. Students worked on their projects on their computers and their work was not as easy to see, even though the professors tried to impose a “work in studio” rule. The workflow and desk crits now used in design studio for Clemson Architecture + Health students is on a group Zoom using Miro Boards and/or live shared screens to navigate within a digital domain with design software (Sketch Up, Revit, Rhino, etc.). This allows students to see each other’s work and hear the feedback that others receive. The increased use of virtual tools to share work in progress has facilitated some of the peer-to-peer learning that I have been missing. Hopefully, in the future we can maintain this way of collaborating and sharing with digital tools while also building the connections and camaraderie that time spent together in studio engenders.
Dr. Anjali Joseph, a faculty member in the Architecture + Health program has responded to the challenge of promoting student engagement and learning in her virtual seminar course by ‘flipping the classroom.’ In the past, she or other industry experts would deliver a lecture on various topics related to healthcare policy and the built environment during the 2.5-hour class. Now part of the lecture is recorded in advance and students spend most of the time in class actively discussing the topic. Dr. Joseph is also using Miro as a way of capturing student reactions to different issues which helps facilitate discussion. This format makes for a more engaging virtual classroom. She feels she will continue to use this format even after we return to in-person instruction.
Communication for Research
Research in healthcare design often involves facility visits to observe healthcare teams at work or to collect data through interviews, surveys and focus groups. Since the start of the pandemic, on-site data collection has been impossible. However, healthcare design researchers in academia as well as practice have adapted by using virtual reality and online surveys or by training healthcare staff to collect data on their behalf. For example, for our deep dive study on anesthesia workspace design, we decided to use video data (collected for another project prior to the pandemic) to understand the nuances of anesthesia medication administration activities and interactions with equipment and space. Architecture firms are increasingly using virtual reality platforms to ‘mock-up’ spaces so clients can experience different design options from various perspectives and provide feedback. During the pandemic, these virtual mock-up evaluations have replaced simulation-based evaluation of physical mock-ups. Virtual mock-ups are challenging in terms of being able to involve multiple individuals in team-based tasks, and they lack the tactile cues that a physical mock-up provides. However, VR has become a viable short-term solution for envisioning proposed spaces. Perhaps the pandemic will result in greater advancements in virtual reality applications that support user engagement in the design process. Architecture firms are also developing detailed research protocols for data collection that can be reliably implemented by staff at healthcare facilities. For example, staff could be recruited to conduct a post-occupancy evaluation using existing tools. Researchers around the world are working to adapt qualitative and quantitative research methods to pandemic conditions. You can read more about these efforts here – (https://rmsig.aib.world/conducting-research-during-covid-19/)
Communication for Employment
While remote interviews are not new, the way in which communication is changing employment is incomplete without a discussion of the physical work environment. A firm’s office tells us a great deal about its values, efficiency and aesthetic sensibility. The irony of interviewing for a job online is that even though you make every attempt to appear as professional as possible, inevitably a cat walks across the camera, a dog starts barking, or a child enters the room unexpectedly. These informal interactions help us relate to one another on a more personal level, but they alter the formal social norms of the office environment. A classmate noted that trying to interview in person during the pandemic was “weird.” The strangeness of masked and socially distanced interactions creates an awkwardness between strangers that lacks the warmth of a handshake and a smile. In a way, Zoom calls allow this boundary to be crossed, assuming people can sufficiently relax and be themselves on camera, which takes time.
Communication for Fun
At the Center for Health Facilities Design and Testing we are using Slack for group communication and collaboration during the pandemic. It started as an experiment to see if we could replace the ‘conversation by the coffee machine’ with something more digital and informal than email. Having the record of communication in a group forum helps with project management and maintains a strong organizational culture. Personally, I find that the “randomfunstuff” channel in our Slack group provides an outlet for informal engagement. The Slack channel helps us maintain a sense of connectedness, especially since many of us are students who live near campus, but spend most days alone in quarantine. We use the “randomfunstuff” channel to upload pictures of where we live and work, share personal art projects, funny stories, images, and to share birthday and holiday wishes.
During my remote summer work with KMD in California, I enjoyed some firm-initiated photo contests that helped us get to know each other, including best WFH (Work-From-Home) footwear (ranging from funny character slippers to furry heels), and best WFH companion (adorable children, cats, puppies, and even a spider web).
Lessons Learned
Overall, digital tools have facilitated better remote coordination in all scenarios, but they have left many of us with a feeling that something is missing. There is another level of relating to each other that occurs in what sociologist Ray Oldenburg calls the third place. (link: https://www.pps.org/article/roldenburg). It has pushed us to find the maximum potential of remote and work-from-home communication. Perhaps the most important lesson learned is that working from home helps us to better understand how a more diverse physical environment enriches our lives.
I have seen so many heart-breaking stories recently about healthcare workers across the world stretched to the limits of their capacity – providing patient care in incredibly difficult conditions while concerned for their own safety and that of their loved ones. A recent WHO report titled, “Keep healthcare workers safe to keep patients safe,” found that across the world, COVID-19 infections were far greater among healthcare workers as compared to the general population. Burnout among healthcare workers is a persistent and ongoing problem in the United States and worldwide. When we add the immense stress of caring of highly infectious patients and being asked to manage with limited personal protective equipment, it threatens to stretch healthcare workers and our system to breaking point. According to an AHRQ report, more than 50% of clinicians report burnout, and there is an increasing concern regarding this rising trend.
Factors leading to burnout
Clinicians experience burnout due to the stressful work environments; a recent report from the national academies of science identified excessive workload, administrative burden, workflow, interruptions, and distractions as factors leading to clinician burnout. Burnout in healthcare providers affects both mental and physical health and leads to high turnover; burnout also impacts hospital outcomes and leads to lower patient satisfaction. A recent survey by Medscape suggests that COVID-19 is increasing physician burnout.
Dealing with stress and burnout
Clinicians utilize many methods to deal with work stress and prevent burnout. According to the literature, clinicians primarily use mindfulness and cognitive training to prevent burnout. Other interventions to prevent clinician burnout include spirituality training, mediation, music therapy, resilience training, and yoga. Although found helpful, these methods also require additional time for training and fitting into the clinician’s already busy schedule. The physical environment is an important factor impacting stress and many other factors contributing to burnout. Thus, we must actively consider the role of the physical environment in reducing burnout among healthcare providers.
Supporting clinicians through environmental design
As designers, we can potentially impact clinician’s burnout directly through improving nature views, daylight access, and improved acoustic conditions in the hospital environment. Designers can also improve workspace ergonomics, and the unit design. Further, environmental design can impact clinician burnout indirectly by helping reduce interruptions, distractions, perceived workload, and work-related injuries.
Access to nature
Window views to nature have restorative and healing effects on patients. Clinicians who have higher access to nature views in their workspace, experience better mood, and lower stress levels. Walking in hospital gardens during clinician breaks has also been associated with reduced burnout levels. Indoor plants, artwork representing nature views, and materials suggesting a link to nature are also among elements that decrease stress and improve clinician job satisfaction. Improving visual quality was more highly valued in hospital break areas in comparison to working spaces.
Daylight
Daylight and exterior views also impact clinician outcomes; operating room staff who had access to exterior views and daylight had considerably lower perceived stress. Exposure to windows and daylight has been linked with reduced blood pressure, improved circadian rhythm, and a restorative effect on acute care clinicians. There is also an indirect relationship between daylight access and clinician burnout. According to research, daylight exposure impacts work-related stress and job satisfaction and is found to impact clinician burnout.
Acoustic environment
Excess noise in clinicians working and resting environments can lead to getting distracted, interrupted and can result in added job workload. A noisy environment can also impair concentration and communication and increase clinician stress levels. Design decisions regarding improving acoustical conditions both in the clinician’s work environment and their resting area may improve outcomes for clinicians.
Ergonomics and furniture
Work-related physical discomfort is prevalent among clinicians and especially surgeons; work-related injury and pain are among factors impacting the surgeon’s burnout and turnover. An ergonomic workplace ideally would provide an appropriate setup for clinicians to conduct their tasks comfortably. Another example of furniture design is improving visual and tactile discrimination in the clinicians’ work area by selecting appropriate materials. Selecting proper materials can help clinicians reduce work-related errors. Suitable furniture design can also create a sense of privacy to minimize visual distractions and interruptions. Studies show that back pain and back injuries among clinicians due to movement and transfer of patients is highly prevalent in healthcare settings. Installing ceiling mounted lifts and providing adequate space around patient beds can help in reducing these injuries and improve staff retention.
Physical space layout
The physical layout of the healthcare facility can help reduce clinicians’ stress and burnout. Providing a private escape and a personal space for clinicians close to their working space could help reduce the adverse effects of a stressful work environment’s for both physicians and nurses. Communication and teamwork are among the factors that impact clinician burnout and are also impacted by the design of the physical layout. Hospital unit designs that result in clinicians walking large distances every day could contribute to fatigue and burnout.
Conclusion
While special design changes have been implemented in healthcare settings during the Covid-19 pandemic to minimize the spread of infections from patients to caregivers; there is a critical need to focus on physical environment features that may help reduce stress, fatigue and burnout among clinicians during this stressful time. Access to nature and daylight, improved acoustical conditions, comfortable setup and ergonomic conditions in workspace, and physical layout of space are all among the factors that could potentially ameliorate the effect of added stress and workload and therefore, could prevent clinician burnout.